delta dental appeal form
PO Box 9219. Healthy Smile Healthy You enrollment form Spanish.
New Member Packet Delta Dental
Disputes not submitted on this form or lacking necessary information to resolve.
. Ad Unrivalled Results for Delta Dental Appeal Form - Are You Ready. DeltaCare USA participation packet request. Delta Dental PPO and Delta Dental Premier network dentists submit claim forms automatically on behalf of Delta Dental patients.
Delta Dental Premier Network Forms - Professional Application Credentialing form Delta Dental Premier Dentists Agreement Ownership Control Form and W-9. Group number dentist license dentist phone no. Delta Dental HIPAA Form 14a Risk Groups.
No yes ifyes enter brief description and. Submit this form if youre. Removable prosthodontics assessment form.
This is the same DC 37 Health Security dental benefit that was provided before the change to Delta Dental. Farmington Hills MI 48333-9219. Dentist directory update form.
Staple x-rays to form-0016-04-10 employee must complete items 1 through 15 last first zip code 6. Delta Dental of Arizona. CLAIMS APPEALS SHOULD BE SENT TO THE STREET ADDRESS BELOW NOT THE PO BOX.
You can download this form insert the necessary information and print it or you can print it and fill in the applicable information. We would like to show you a description here but the site wont allow us. Delta Dental HIPAA Form 14b ASO Groups.
Employee subscriber name employee home address city state zip 10. Dentist Forms - Delta Dental Mass Dentists Forms Direct Deposit Form W-9 from the Internal Revenue Service Individual plan brochure order form CredentialingRecredentialing. Delta dental of new york inc.
Locum tenens provider form. Employer company name and address. You can also choose within this packet to join the Delta Dental PPO network at the same time.
New York Inc Delta Dental of Pennsylvania and Delta Dental Insurance Company together with our affiliate companies form one of the nation. Delta Dental PPO participation packet request. With Delta Dental we keep you smiling.
Group Plan Appeals. THE PO BOX IS FOR CLAIMS ONLY. Healthy Smile Healthy You enrollment form.
And i request predetermination of benefits treatment completed. Disputes must be written and must clearly describe the basis of the dispute. Group Claim Form This claim form is for Delta Dental PPO Delta Dental Premier and non-network claims.
Use this secure form to file a grievance or appeal a dental benefits decision. Box 2105 mechanicsburg pa 17055-6999 717 766-8500 800 932-0783. We have 1 business day after we receive the information from the treating provider to decide whether we should change our decision and authorize your requested service.
ASO contract addendum for HIPAA privacy and security. Dentist Administrative Forms and Resources. Staple x-rays to form form ddny-0016-04-10 employee must complete items 1 through 15 last first zip code 6.
Theres no hassle in working through claims saving you time and frustration. Dentist participants residing in NY State or a Delta Dental PPO dentist participants residing outside NY State up to the 1700 annual maximum per eligible participant. Termination request form We require written notification when you close a service office or terminate your network membership.
Check Hot Trending Viral Search Suggestions for Delta Dental Appeal Form. If you wish to file a dispute with Delta Dental please complete the form below include all supporting documentation and clearly identify why you are disputing Delta Dentals action or inaction. Automatic bank draft authorization for risk groups.
Employer company name and address 1. Group Information Change Request Form. Please refer to the vision appeals packet for information on submitting DeltaVision Administered by EyeMed appeals.
The Senior Grievance and Appeals Coordinator will communicate vitals and prioritization and clear obstacles preventing appeal and grievance front line team members from achieving targets each day. Review the Member Dentist Rules and Regulations. Appeal Form - Information on how to appeal your claim.
Does the DC 37 Health Security Delta Dental. Istreatment result of occupational illness or injury. Through our national network of Delta Dental.
CLAIMS APPEALS SENT TO THE PO BOX WILL BE DELAYED. Continuous orthodontic coverage form for DeltaCare USA.

The Following Provider Types Should Bill Using The Dental Claim Form Pdf Free Download
2

Confused By Dental Insurance We Have The Answers Mcomie Dentistry

Hawk I Orthodontic Network Forms Delta Dental Of Iowa
2

News Release Delta Dental Of Wisconsin
2
2
2
2
2
Delta Dental Insurance
2
2
2
2
Delta Dental Ppo Ucnet University Of California
2
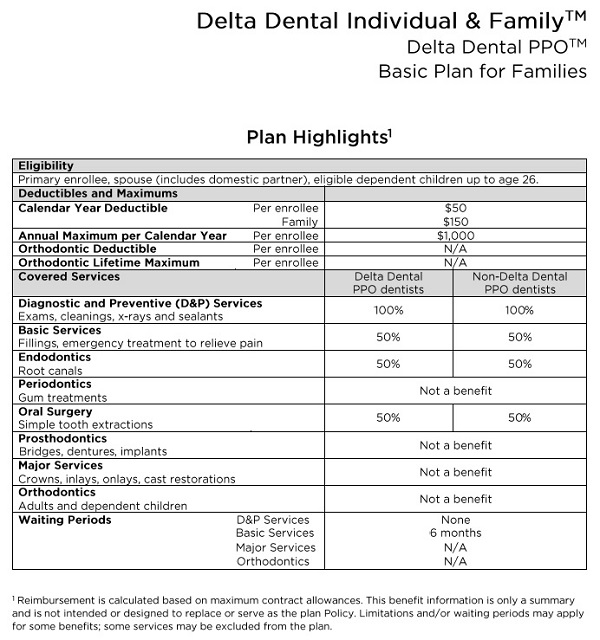
Delta Dental Individual Family Plans For 2019